Occurs in 20-50% women (especially in perimenopausal age)
Symptomatology:
a.u.b. (abnormal menstrual and intermenstrual uterine bleeding)
Sense of weight and pelvic pain
Volumetric increase at subsequent controls
Compression symptoms (feeling of weight)
Sterility or abortive
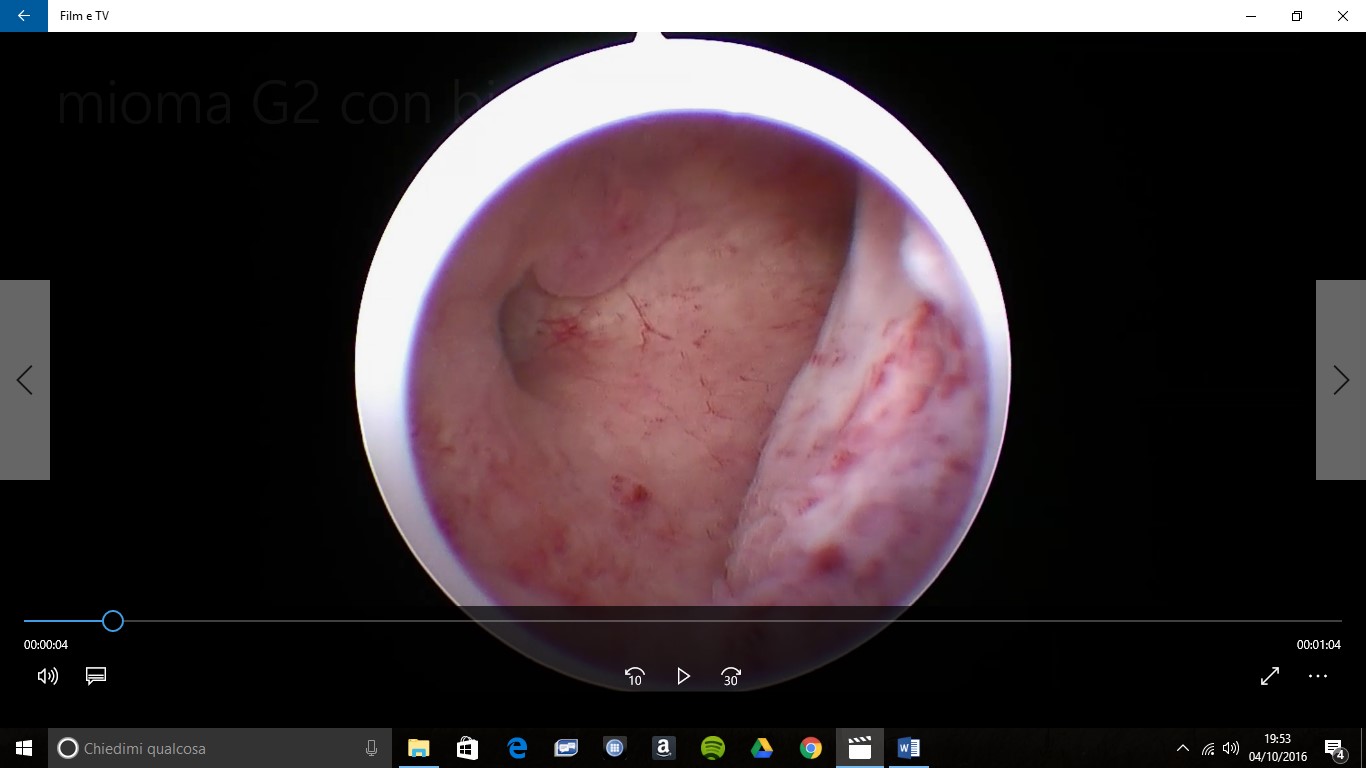
Myomas of hysteroscopic relevance are only submucosal ones that are divided into:
G0 myoma: completely endocavitary myoma
G1 and G2 myoma with more or less than 50% intrauterine development.
When is it necessary to operate on a submucosal myoma?
Always if a woman wishes to become pregnant (the presence of a myoma can cause sterility or miscarriages)
Always if it is symptomatic (i.e. if it causes continuous, heavy menstruation, bleeding outside menstruation)
Before operating on a submucosal myoma, it is essential to determine its size, location, number, intramural development, distance from the external surface of the uterus
Pre-surgical diagnosis and evaluation is done with:
A) Outpatient hysteroscopy, which allows evaluation:
The intracavitary portion of the myoma
Its location
The characteristics of the endometrium
Any associated intracavitary pathologies
B) Transvaginal ultrasound or sonohysterography allows the evaluation of
The actual size of the myoma and the location especially if it is intramural
The 'myometrial free margin', i.e. the thickness of the myometrium above the myoma
The presence of other associated pathology (subserous myomas, ovarian cysts
Submucosal myoma
Submucosal myoma
Submucosal myoma
Myoma I.M. Fundico
The operating technique must have the following objectives
Total removal of myoma
Respect for uterine anatomical integrity
It recognises the following phases
G0 myoma: resection of the myoma until its complete removal
G1 and G2 myomas: resection of the endocavitary part with thermal loops and of the intramural part with cold loops, a complex operation depending on whether the development is partially or predominantly intramural and which requires proven operator skill and the use of various types of loops with different functions
Complete removal of the myoma in no more than two stages. Any other solution proposed or implemented carries the risk of not resolving the symptoms.