They can have cancerous cells inside in 0.2-10 % of cases depending on whether the woman is in her childbearing years or menopausal
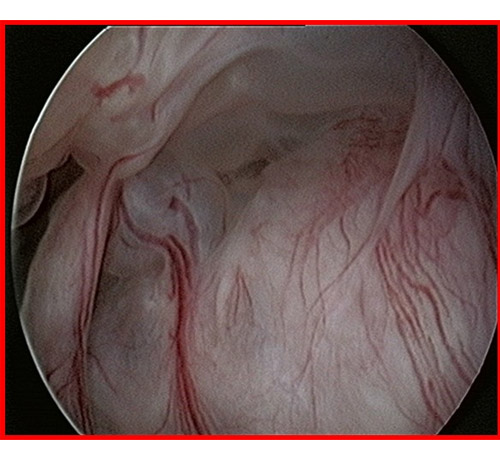
It is a frequent condition and the main cause of abnormal uterine bleeding. They may be asymptomatic and only suspected during a gynecological examination with ultrasound. It is essential to make a diagnosis of certainty with a diagnostic hysteroscopy
Endocervical polyps are referred to as 'sentinel polyps' because in 25% of cases they are the telltale sign of the presence of another cervical polyp behind it or of an endometrial polyp inside the uterus. This is why today it is no longer permissible to remove a polyp with forceps as was once done, but it is compulsory to perform a diagnostic hysteroscopy and remove it with a hysteroscopic resection
Practicable in the surgery if less than 1-1.5 cm.
Hysteroscopic resection of an endometrial or cervical polyp should be performed within the first half of the cycle if the woman is menstruating, at any time if she is menopausal.
Execution Technique
Objectives:
Complete removal of the polyp including the implant base.
Instrumentation required:
Bipolar or monopolar mini-receptor for polyps larger than 15 mm
Continuous-flow office hysteroscope with micropincers, microscissors and bipolar electrod for resecting polyps smaller than 15 mm without anaesthesia in the outpatient clinic